CPC Certified Professional Coder (CPC) Exam Questions and Answers
A complete cardiac MRI for morphology and function without contrast, followed by contrast with four additional sequences and stress imaging, is performed on a patient with systolic left ventricular congestive heart failure and premature ventricular contractions.
What CPT® and ICD-10-CM codes are reported?
A planned partial meniscectomy of the temporomandibular joint is cancelled after anesthesia and incision due to respiratory distress.
What CPT® coding is reported for the oral surgeon?
A physician excises a 3.5 cm malignant lesion including margins from the back. Then a destruction of a 2.0 cm benign lesion on the right cheek of the face with cryosurgery.
What CPT@ and ICD-10-CM is reported?
View MR 006399
MR 006399
Operative Report
Preoperative Diagnosis: Chronic otitis media in the right ear
Postoperative Diagnosis: Chronic otitis media in the right ear
Procedure: Eustachian tube inflation
Anesthesia: General
Blood Loss: Minimal
Findings: Serous mucoid fluid
Complications: None
Indications: The patient is a 2-year-old who presented to the office with chronic otitis media refractory to medical management. The treatment will be eustachian tube inflation to remove the fluid. Risks, benefits, and alternatives were reviewed with the family, which include general anesthetic, bleeding, infection, tympanic membrane perforation, routine tubes, and need for additional surgery. The family understood these risks and signed the appropriate consent form.
Procedure in Detail: After the patient was properly identified, he was brought into the operating room and placed supine. The patient was prepped and draped in the usual fashion. General anesthesia was administered via inhalation mask, and after adequate sedation was achieved, a medium-sized speculum was placed in the right ear and cerumen was removed atraumatically using instrument with operative microscope. The tube is dilated, an incision is made to the tympanum and thick mucoid fluid was suctioned. The patient was awakened after having tolerated the procedure well and taken to the recovery room in stable condition.
What CPT® coding is reported for this case?
A patient undergoes a percutaneous liver biopsy with ultrasound guidance for primary biliary cirrhosis.
What CPT® and ICD-10-CM codes are reported?
A 1-year-old patient has bilateral supernumerary digits:
Left digit contains bone and joint → amputated
Right digit is a soft-tissue nubbin → simple excision
What CPT® coding is reported?
A patient with empyema requires a Schede thoracoplasty.
What CPT® code is reported for this procedure?
(A patient presents to the urgent care facility with multiple burns acquired while burning debris in his backyard. After examination the physician determines the patient hasthird-degree burns of the left and right posterior thighs (10%). He also hassecond-degree burnsof theanterior portion of the right side of his chest wall (8%)andupper back (6%).TBSA is 24%withthird-degree burns totaling 10%. What ICD-10-CM codes are reported, according to ICD-10-CM coding guidelines?)
(A 55-year-old female with severe coronary arteriosclerosis with angina is admitted for elective coronary artery bypass. The surgeon performed a coronary artery bypass using asaphenous vein harvested endoscopically. The vein graft was anastomosed to theobtuse marginaland theleft circumflex. What CPT® coding is reported for this procedure?)
In medical terminology, suffixes indicate the procedure, condition, disorder, or disease.
Which term contains a suffix?
(A patient is in her dermatologist’s office for treatment of recurring psoriatic plaques on the upper back and neck resistant to topical therapy. The dermatologist performsExcimer laser therapyon the upper back (300 sq cm) and neck (100 sq cm), total surface area400 sq cm. What CPT® codes are reported?)
A patient presents for planned sterilization via bilateral excisional vasectomy.
What CPT® and ICD-10-CM codes are reported?
A cardiologist attempted to perform a percutaneous transluminal coronary angioplasty of a totally occluded blood vessel. The surgeon stopped the procedure because of an anatomical problem creating risk for the patient and preventing performance of the catheterization.
What modifier is appended to the procedure code?
The evisceration of ocular contents was performed using a surgical microscope for enhanced visualization. The procedure was performed on the left eye and an implant was not placed in the ocular cavity.
What CPT® coding is reported?
(A 52-year-old woman has vulvar intraepithelial neoplasia (VIN II). The surgeon performs avulvectomyremovingless than 80%of the vulva, including affected skin and deep subcutaneous tissue. What CPT® and ICD-10-CM codes are reported?)
A patient undergoes MRI-guided needle liver biopsy with two core samples taken.
What CPT® codes are reported?
A patient is sent to the hospital by his family care provider for admission due to a high fever and neck pain The patient is admitted to the hospital to rule out bacterial meningitis. The hospitalist admits the patient and orders a CBC. CMR Blood culture, CT of the head and chest, and a lumbar puncture (spinal tap). After review of the results, he determines the patient has bacterial meningitis and starts the patient on IV antibiotics.
What CPT® and ICD-10-CM codes are reported for the admission?
A 3-day-old died in her sleep. The pediatrician determined this was the result of crib death syndrome. The parents give permission to refer the newborn for a necropsy. The pathologist receives the newborn with her brain and performs a gross and microscopic examination. The physician issues the findings and reports they are consistent with a normal female newborn.
What CPT® code is reported?
Four malignant peritoneal tumors are excised, the largest measuring 15 cm.
What CPT® and ICD-10-CM coding is reported?
A patient undergoes angioplasty with stent placement in the left iliac artery.
What CPT® coding is reported?
A patient had surgery a year ago to repair two extensor tendons in his wrist. He is in surgery for a secondary repair for the same two tendons with free graft. What CPT® coding is reported?
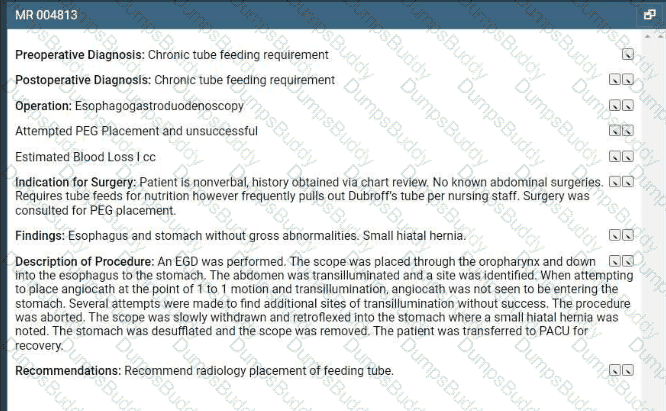
Refer to the supplemental information when answering this question:
View MR 004813
What CPT® and ICD-10-CM codes are reported?
A 10-year-old had a cochlear implant in his left ear few weeks ago. Today he sees the audiologist to initialize and program the implant.
What CPT® code is reported?
A 42-year-old male is diagnosed with a left renal mass. An abdominal incision along with rib resection is made to expose and access the kidney. The left kidney is removed, along with surrounding fat, adrenal gland, lymph nodes in the area, and the incision site is sutured. What CPT ® code is reported for this procedure?
Which place of service code is submitted on the claim for a service that is performed in an outpatient surgical floor?
What does the term “manipulation” refer to in the context of fracture or dislocation treatment?
(A 60-year-old man presents for examination of the entire rectum andsigmoid colon. Two polyps are found in the sigmoid colon and removed usingablation. What CPT® and ICD-10-CM codes are reported?)
A 50-year-old patient presented with a persistent cough has not responded to standard treatments. The patient ' s physician decides to perform a flexible bronchoscopy with bronchial biopsies to further investigate the cause. A flexible bronchoscope is inserted through the patient ' s mouth and into the bronchial tubes. Five biopsies are taken for further testing. The biopsies were sent to the lab for analysis to determine the next steps in the patient ' s treatment plan.
What CPT® coding is reported?
(The patient presents to the emergency department with chest pain. EKG showsNSTEMIand troponin is abnormal. The ED provider discusses the case with a cardiologist and the patient is admitted for heart catheterization/PCI. What is the E/M service and ICD-10-CM coding reported for the ED provider?)
A 20-year-old female is being seen for the first time by a primary care physician to have a yearly physical. During the examination for the physical, the provider discovers non-inflammed lesions on her legs and arms. The physician performs a complete physical and additional separate documentation for the treatment of the lesions on the bilateral upper and lower extremities. The provider has the patient buy an over-the-counter ointment and will continue to watch them.
What CPT® coding is reported for this visit?
(A 42-year-old female is in the operative room to repair azone 2 flexor digitorum profundus (FDP) tendonlaceration involving her index finger with an associatedradial digital nerveinjury. The dorsal side of the FDP tendon was sutured. Next, themicroscopewas brought into place and the radial digital nerve was repaired using epineural sutures. What CPT® codes are reported?)
A patient is diagnosed with a healing pressure ulcer on her left heel that is currently being treated.
What ICD-10-CM coding is reported?
A pediatrician is requested to attend a high-risk delivery and performs initial stabilization of the newborn after cesarean delivery.
What E/M service is reported?
An anesthesiologist medically directs two cases during EGD and colonoscopy in a PS III patient with severe bleeding risk.
What CPT® codes are reported?
(A patient presents with dysuria and lower abdominal pain. The physician suspects UTI. Anautomated urinalysis without microscopyis done in the office and isnegative. UTI is ruled out for the final diagnosis. What CPT® and ICD-10-CM codes are reported?)
A patient is seen at the doctor ' s office for nausea, vomiting, and sharp right lower abdominal pain. CT scan of the abdomen is ordered. Labs come back indicating an increased WBC count with
review of the abdominal CT scan. The physician determines the patient has chronic appendicitis. The physician schedules an appendectomy and takes the patient to the operating room. The
appendix is severed from the intestines and removed via scope inserted through an umbilical incision. What CPT® and diagnosis codes are reported?
(A 14-month-old male with a unilateral complete cleft lip and alveolar cleft palate had prior repair of the cleft lip. He now presents forreconstruction of the palatewith closing the fissure in the soft tissue of thealveolar ridge with bone graft. What CPT® coding is reported?)
A patient is diagnosed with sepsis due to enterococcus. What ICD-10-CM code is reported?
(A wheelchair-bound resident of a skilled nursing facility is seen in the physician’s office. The physician’s office makes arrangements with a social worker to take the patient back to the skilled nursing facility. What is the HCPCS Level II transportation service code?)
(A patient is diagnosed with agangrenous ulceron theright thighwith thefat layer exposedand is currently being treated. What ICD-10-CM coding is reported?)
A patient presents to the pulmonologist ' s office for the first time with coughing and shortness of breath. The patient has a history of asthma. The physician performs a medically appropriate
history and exam. The following labs are ordered: CBC, arterial blood gas, and sputum culture. The pulmonologist assesses the patient with a new diagnosis of COPD. The patient is given a
prescription for the inhaler Breo Ellipta.
What E/M code is reported?
(A patient has nausea with several episodes of emesis and severe stomach pain due to dehydration. Normal saline is infused in the same bag with2 mg ondansetron. Then15 mg ketorolac tromethamineis given for stomach pain. What J codes are reported for these services?)
(A patient is in her otolaryngologist’s office to receive therapeutic treatment forasthmatic bronchitis with status asthmaticus. A subcutaneous injection ofomalizumab (150 mg)is given in her left upper arm. What is the CPT® and ICD-10-CM coding?)
Mr. Woolridge has had a suspicious lesion on his left shoulder for approximately eight weeks that is not healing. On the dermatologist ' s exam of left shoulder blade, there is excoriation and scabbing and the lesion not healing. Patient agrees and wishes to proceed with a punch biopsy of the lesion. A punch biopsy is taken of the lesion and sent to pathology. A simple repair is performed at the biopsy site.
What CPT® and ICD-10-CM codes are reported?
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® and ICD-10-CM code is reported?
A child returns for stage 2 surgical repair of double outlet right ventricle, including removal of pulmonary artery band, arterial switch repair, and ECMO cannulation.
What CPT® codes are reported?
A 5-year-old patient has a fractured radius. The orthopedist provides moderate sedation and the reduction. The time is documented as 21 minutes.
What CPT® code is reported for the moderate sedation?
A 30-year-old patient with a scalp defect is having plastic surgery to insert tissue expanders. The provider inserts the implants, closes the skin, and increases the volume of the expanders by injecting saline solution. Tissue is expanded until a satisfactory aesthetic outcome is obtained to repair the scalp defect.
What CPT® code is reported?
A patient is brought to the operating room with a right-sided peripheral vertigo. The provider makes a postauricular incision and uses an operating microscope to perform a mastoidectomy using a burr. He next destroys the semicircular canals, the utricle, and saccule completely removing the diseased labyrinth structures. The provider sutures the incision.
What CPT® code and ICD-10-CM codes are reported?
A 45-year-old female presents to the ED with chest pain. The provider has an Albumin Cobalt Binding Test to determine if the chest pain is ischemic in nature.
That lab test is reported?
A 55-year-old patient was recently diagnosed with an enlarged goiter. It has been two years since her last visit to the endocrinologist. A new doctor in the exact same specialty group will be examining her. The physician performs a medically appropriate history and exam. The provider reviewed the TSH results and ultrasound. The provider orders a fine needle aspiration biopsy which is a minor procedure.
What E/M code is reported?
(Full Case:Location:ABC Outpatient Clinic.Patient:60-year-old menopausal female.Independent radiologist (not employed by hospital):Dr. Q.Chief complaint:Uterine cramping.Procedure:Transvaginal ultrasound.Findings:Ovaries normal; measurements given (note: left ovary listed twice with different dimensions); uterus 5.2 × 5.1 × 4.0; endometrial stripe 0.8 cm; uterus without focal hypoechoic mass; ovoid anechoic foci in lower uterus/cervix due to Nabothian cysts; no adnexal fluid or mass; cervix thickness/length normal; true sagittal thickest portion measured.Question:What CPT® and ICD-10-CM codes are reported for the independent radiologist that provided the interpretation of the ultrasound?)
A patient undergoes CABG using the right internal mammary artery anastomosed to three coronary arteries.
What CPT® coding is reported?
(A 1-year-old patient was born with twosupernumerary digits, one extending from the right pinky and one extending from the left pinky. The digit from his left pinky is larger and includes themetacarpal bone with a jointand is amputated. The one on the right is anubbinand containsno bony structure. The hand surgeon removes the extra digit containingsoft tissueby a simple excision. What is the CPT® coding for the procedures performed?)
(ESTABLISHED PATIENT VISIT: A 37-year-old woman presents with coughing, congestion, upper respiratory symptoms, and headache for two days. Complete ROS negative except as noted. No significant past/family history. Exam: stable vitals, nasal congestion, normal TMs, occasional rhonchi, no wheezing, normal heart, soft abdomen. Assessment/Plan:Acute upper respiratory infection, fluids,amoxicillinfor 5–7 days, return precautions. What CPT® code is reported?)
What modifier is appended to indicate when a procedure performed during the postoperative period is unrelated to the original surgery?
(A patient presents for surgery due to recurrent lumbar radiculopathy at a previously operated spinal level. The surgeon performs arepeat exploration laminotomywithbilateral foraminotomyto decompress nerve roots at theL1–L2 interspace. No additional spinal levels are treated. What CPT® coding is reported?)
A patient with jaundice was seen by the physician to obtain liver biopsies. A needle biopsy was taken using CT guidance for needle placement. The physician obtained two core biopsies, which
were then sent to pathology. What CPT® codes are reported?
A 63-year-old is seen by his. primary care physician for an annual exam. His last exam with the primary care physician was four years ago. He has no complaints.
What CPT code is reported?
(The documentation states: “A punch is placed and pushed downward to obtain a tissue sample for a biopsy of thelunula.” What anatomical structure is being biopsied?)
A 60-year-old male has three-vessel disease and supraventricular tachycardia which has been refractory to other management. He previously had pacemaker placement and stenting of LAD coronary artery stenosis, which has failed to solve the problem. He will undergo CABG with autologous saphenous vein and an extensive modified MAZE procedure to treat the tachycardia.
He is brought to the cardiac OR and placed in the supine position on the OR table. He is prepped and draped, and adequate endotracheal anesthesia is assured. A median sternotomy incision is made and cardiopulmonary bypass is initiated. The endoscope is used to harvest an adequate length of saphenous vein from his left leg. This is uneventful and bleeding is easily controlled. The vein graft is prepared and cut to the appropriate lengths for anastomosis. Two bypasses are performed: one to the circumflex and another to the obtuse marginal. The left internal mammary is then freed up and it is anastomosed to the ramus, the first diagonal, and the LAD. An extensive maze procedure is then performed and the patient is weaned from bypass. At this point, the sternum is closed with wires and the skin is reapproximated with staples. The patient tolerated the procedure without difficulty and was taken to the PACU.
Choose the procedure codes for this surgery.
(A patient presents for evaluation of suspicious skin lesions. During the encounter, the provider performs:
• Incisional biopsy of adeep inflammatory lesionon the upper arm
• Punch biopsy of aseparate lesionon the forearm
• Shave biopsy of asuperficial lesionon the shoulder
Each biopsy is performed on a separate lesion for diagnostic purposes, and all specimens are submitted to pathology. What CPT® coding is reported?)
Which place of service code is submitted on the claim for a service that is performed in a skilled nursing facility?
(A 32-year-old visited a provider due to ongoing irritation and watering in his left eye. Suspecting an allergy, the provider carried out a test, introducing an allergenic extract into the mucous membrane inner lining of the eye. The patient’s eye is monitored for signs of an allergic reaction, such as redness and itching. What CPT® code is reported?)
A 4-year-old, critically ill child is admitted to the PICU from the ED with respiratory failure due to an exacerbation of asthma not manageable in the ER. The PICU provider takes over the care of the patient and starts continuous bronchodilator therapy and pharmacologic support with cardiovascular monitoring and possible mechanical ventilation support.
What is the E/M code for this encounter?
The patient came in with an inflamed seborrheic keratosis on her nose for a shave removal. After applying local anesthesia, a 0.7 cm dermal lesion was removed using an 11 blade.
What CPT® and ICD-10-CM codes are reported?
A provider orders liquid chromatography mass spectrometry (LC-MS) definitive drug test for a patient suspected of acetaminophen (analgesic) overdose. What CPT® code is reported for the test?
(A 32-year-old is in the outpatient clinic for anesophagoscopydue to increased difficulty swallowing with hiseosinophilic esophagitis. The flexible scope is inserted into the esophagus. Examination notes narrowing in the distal esophagus. Following an injection of Kenalog, atransendoscopic balloon dilationis performed in the area of stenosis, eventually reaching 18 mm. What CPT® coding is reported for this procedure?)
A couple presents to the freestanding fertility clinic to start in vitro fertilization. Under radiologic guidance, an aspiration needle is inserted (by aid of a superimposed guiding-line) puncturing the ovary and preovulatory follicle and withdrawing fluid from the follicle containing the egg.
What is the correct CPT® code for this procedure?
A comatose patient is seen in the ER. The patient has a history of depression. Drug testing confirm she overdosed on tricyclic antidepressant drugs doxepin, amoxapine, and clomipramine.
What CPT® code is reported?
What CPT® coding is reported for a subtotal thyroidectomy for malignancy with radical neck dissection?
(Full Case:Procedure:Excision of6.0 cm malignant lesionof theright forearmwithadjacent tissue transferusing arotation flap.Pre/Post-op Dx:Basal cell carcinoma, right forearm.Anesthesia:local (1% Xylocaine with epi).Defect size:8 sq cm.Specimen:sent forfrozen section margin control; margins confirmed clear.Closure:rotation flap from adjacent healthy tissue,total area 8 sq cm, secured with layered closure (5-0 Vicryl/6-0 Prolene).Question:What CPT® coding is reported?)
A patient undergoes cystourethroscopy with pyeloscopy and manipulation to remove a ureteral calculus. No stent is inserted.
What CPT® coding is reported?
A 55-year-old patient with suspected liver cancer was seen by the physician to obtain a biopsy. The special biopsy needle was placed using ultrasonic guidance. The physician obtained a small tissue sample from the liver, which was then sent to pathology.
What CPT® codes are reported?
A woman at 36-weeks gestation goes into labor with twins. Fetus 1 is an oblique position, and the decision is made to perform a cesarean section to deliver the twins. The obstetrician who delivered the twins, provided the antepartum care, and will provide the postpartum care.
What CPT® coding is reported for the twin delivery?
A patient who has colon adenocarcinoma undergoes an open partial colectomy. The surgeon removes the proximal colon and terminal ileum and reconnects the cut ends of the distal ileum and
remaining colon.
What procedure and diagnosis codes are reported?
Which circumstance supports medical necessity for a payment by the insurance company?
A therapeutic colonoscopy is performed, where the scope goes beyond the splenic flexure, but not to the cecum. Using the Colonoscopy Decision Tree illustrated in the CPT® code book, what coding is reported?
A 42-year-old male is diagnosed with a left renal mass. Patient is placed under general anesthesia and in prone position. A periumbilical incision is made and a trocar inserted. A laparoscope is inserted and advanced to the operative site. The left kidney is removed, along with part of the left ureter. What CPT® code is reported for this procedure?
A patient arrived at the emergency department experiencing pain in both legs. The ED physician ordered a comprehensive duplex scan of the arteries in both lower extremities to rule out arteriosclerosis.
What CPT® and ICD-10-CM codes are reported?
A 58-year-old with type 1 diabetes mellitus comes in for comprehensive eye examination. She is diagnosed with diabetic retinopathy with macular edema in the right eye. What ICD-10-CM coding is reported?
The provider performs a radical resection of a 4.5 cm sarcoma in the upper arm.
What CPT® coding is reported?
The CPT® code book provides full descriptions of medical procedures, although some descriptions require the use of a semicolon (;) to distinguish among closely related procedures.
What is the full description of CPT® code 69644?
A patient arrives with stridor and in respiratory distress. The provider performs a micro laryngoscopy using a Parson ' s laryngoscope and magnifying telescope. A bronchoscopy was also
performed using a 2.5 Stortz bronchoscope. The findings include subglottic web and stenosis with laryngeal edema suggestive of reflux. There was also significant collapse of the trachea at
the carina and into the main bronchi bilaterally.
What CPT® coding is reported?
A 19-year-old is seen by his, primary care physician for an annual exam. His last exam with the primary care physician was four years ago. He has no complaints.
What CPT code is reported?
Dr. Carter sees Mrs. White at the Spring Valley Nursing Facility. He saw her last month after she was admitted to the facility. Today is a follow up visit. She is doing well. He documented a medically appropriate history and exam. The patient has osteoporosis, hypertension, dementia. CAD, CHF, and type 2 diabetes (moderate number and complexity of problems). He reviews 4 labs and a telemetry (Moderate data). He adds a Cardizem prescription for better control of her blood pressure which is a moderate risk. What CPT® code does Dr. Carter report for the visit?
(Miranda is in her provider’s office for follow up of her diabetes. Her blood sugars remain at goal with continuing her prescribed medications. When referring to the MDM Table for number and complexity of problems addressed, what type of problem is this considered?)
A 45-year-old patient comes In with chronic sinusitis that has not responded to medication. The physician decides to use a sinus stent implant to help alleviate the patients symptoms.
The physician inserts the implant into the ethmoid sinus using a delivery system. This implant is designed to keep the surgical opening clear, prop open the sinus, and gradually release a corticosteroid with anti-inflammatory properties directly to the sinus lining. The implant is not permanent and will dissolve over time.
What HCPCS Level II code is reported?
A healthy 35-year-old undergoes EP study and ablation under general anesthesia.
What anesthesia coding is correct?
A 23-year-old receives MMR and Hepatitis B vaccines without counseling.
What CPT® codes are reported?
A patient underwent a cystourethroscopy with a pyeloscopy using lithotripsy to break up the ureteral calculus. An indwelling stent was also inserted during the same operative session on the same side. This service was performed in the outpatient hospital surgery center.
What CPT® coding reported?
A 5-year-old who has an allergy history experienced a possible reaction to peanuts. A quantitative, high-sensitive fluorescent enzyme immunoassay was used to measure specific IgE for recombinant peanut components. Results showed there was no reaction indicating the child has a peanut allergy.
What lab test is reported?
A cardiologist performs and interprets a 12-lead ECG in the office.
What CPT® coding is reported?
A 58-year-old male suffered an acute STEMI of the inferolateral wall while running a marathon on June 15 and had received treatment. Three weeks later, the patient presents to the ED complaining of SOB and left arm pain. An EKG is performed as well as blood tests. Patient is admitted for further evaluation.
What diagnosis code is reported for this encounter?
A patient is seen at the doctor ' s office for nausea, vomiting, and sharp right lower abdominal pain. CT scan of the abdomen is ordered. Labs come back indicating an increased WBC count with review of the abdominal CT scan. The physician determines the patient has a ruptured appendicitis. The physician schedules an appendectomy and takes the patient to the operating room. The appendix is severed from the intestines and removed via scope inserted through an umbilical incision. What CPT® and diagnosis codes are reported?
A patient presents with recurrent spontaneous episodes of dizziness of unclear etiology. Caloric vestibular testing is performed irrigating both ears with warm and cold water while evaluating the patient’s eye movements. There is a total of three irrigations.
What CPT® coding is reported?
A provider performs a mastoidectomy and complete labyrinthectomy for right-sided peripheral vertigo.
What CPT® and ICD-10-CM codes are reported?
Patient had polyps removed on a previous colonoscopy. The patient returns three months later for a follow-up examination for another colonoscopy. No new polyps are seen.
What diagnosis coding is reported for the second colonoscopy?
Which HCPCS Level II codes identify temporary services that would not be assigned a CPT® code, but are needed for claims processing purposes?
The surgeon performs Roux-en-Y anastomosis of the extrahepatic biliary duct to the gastrointestinal tract on a 45-year-old patient.
What CPT® code is reported?
View MR 005398
MR 005398
Operative Report
Preoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Postoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Procedure: Right nephrectomy with partial ureterectomy.
Findings and Procedure: Under satisfactory general anesthesia, the patient was placed in the right flank position. Right flank and abdomen were prepared and draped out of the sterile field. Skin incision was made between the 11th and 12th ribs laterally. The incision was carried down through the underlying subcutaneous tissues, muscles, and fascia. The right retroperitoneal space was entered. Using blunt and sharp dissection, the right kidney was freed circumferentially. The right artery, vein, and ureter were identified. The ureter was dissected downward where it is completely obstructed in its distal extent. The ureter was clipped and divided distally. The right renal artery was then isolated and divided between 0 silk suture ligatures. The right renal vein was also ligated with suture ligatures and 0 silk ties. The right kidney and ureter were then submitted for pathologic evaluation. The operative field was inspected, and there was no residual bleeding noted, and then it was carefully irrigated with sterile water. Wound closure was then undertaken using 0 Vicryl for the fascial layers, 0 Vicryl for the muscular layers, 2-0 chromic for subcutaneous tissue, and clips for the skin. A Penrose drain was brought out through the dependent aspect of the incision. The patient lost minimal blood and tolerated the procedure well.
What CPT® coding is reported for this case?
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What E/M code is reported for this encounter?
Refer to the supplemental information when answering this question:
View MR 138093
What E/M coding is reported?
(Which statement accurately reflects CPT® parenthetical guidance for codes69209and69210?)
An abdominal X-ray includes decubitus, supine, and erect views.
What CPT® code is reported?
A surgeon performs midface LeFort I reconstruction on a patient’s facial bones to correct a congenital deformity. The reconstruction is performed in two pieces in moving the upper jawbone forward and repositioning the teeth of the maxilla of the mid face.
What CPT® code is reported?
A patient presents to the labor and delivery department for a planned cesarean section for triplets. She is at 37 weeks gestation. She is given a continuous epidural for the delivery.
What anesthesia coding is reported?
A patient with Parkinson ' s has sialorrhea. The physician administers an injection of atropine bilaterally into a total of four submandibular salivary glands.
What CPT® coding is reported?
(A 62-year-old with insulin-dependent diabetes mellitus has sudden hearing loss. The otolaryngologist administered atranstympanic injection of a steroidfor the sudden hearing loss ineach ear. How is this reported?)
(A patient is seen by her podiatrist to treat a painfulleft ingrown toenailon the big toe. The podiatrist performs awedge excisionof the skin of the nail fold at the lateral margin. Local anesthetic is administered, and an elliptical incision is made through subcutaneous tissue of the affected nail groove. A wedge-shaped piece of soft tissue from the nail margins is removed. What CPT® code is reported?)
(A trauma patient needs the following imaging:2 views nasal bones,3 views chest,2 views left forearm,2 views tibia/fibula. To exclude stroke, aCTA head with contrastis also ordered. What CPT® coding is reported?)
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® codes are reported?
What is the medical term for a procedure that creates an opening between the bladder and the rectum?
A surgeon performs a complete bilateral mastectomy with insertion of breast prosthesis at the same surgical session.
What CPT@ coding is reported?
A patient ' s left eye is damaged beyond repair due to a work injury. The provider fabricates a prosthesis from silicon materials and makes modifications to restore the patient ' s cosmetic appearance.
What CPT® code is reported?
(Full Case:Chief complaint:Syncope.HPI:68-year-old male arrives to ED inrespiratory distressafter sudden syncope/collapse while shopping; unresponsive; EMS: weak pulse, labored respirations, unresponsive. History:CABG 5 years ago, no chest pain since.ROS:unobtainable (unconscious).Allergies:none.Meds:Coumadin.PMH:HTN.Social:lives with wife.Exam/Vitals:BP 82/62, pulse 79, RR 12 shallow, O2 sat 90% on high flow O2; monitor shows right bundle branch block. Neuro: initially eyes closed, opens to questions, responds to some questions, later unresponsive. HEENT pupils sluggish equal; unable EOM/fundus. Neck supple, no JVD/bruits. Lungs mild rhonchi. Heart regular without murmurs. Abdomen benign. Extremities symmetric, no edema/cyanosis. Skin no rash. Neuro no focal deficits.Hospital course:IV x2; NS 1000 cc bolus with little response; dopamine drip 10 → 20 mcg/kg/min; O2 sat drops, respirations slow; becomes unresponsive; progresses tocardiac arrest; CPR; multiple adrenaline/atropine; defibrillation; ABG pH 7.1 etc; bicarbonate x2; no effect; pronounced dead 13:32.Critical care time:77 minutes continuous.Diagnosis:Cardiorespiratory arrest.Question:What is the E/M coding reported for this encounter?)
A patient returns for embryo transfer. The lab thaws cryopreserved embryos and cultures them for two additional days.
What CPT® coding is reported?
Mrs. Wilder presents with right and left leg swelling. Venous thrombosis imaging of each leg is done and shows deep venous embolism and thrombosis in each leg.
What CPT® and ICD-10-CM codes are reported?
A 65-year-old gentleman presents for refill of medications and follow-up for his chronic conditions. The patient indicates good medicine compliance. No new symptoms or complaints.
Appropriate history and exam are obtained. Labs that were ordered from previous visit were reviewed and discussed with patient. The following are the diagnoses and treatment:
Hypokalemia - stable. Refill Potassium 20 MEQ
Hypertension - blood pressure remaining stable. Patient states home readings have been in line with goals. Refill prescription Lisinopril.
Esophageal Reflux - Patient denies any new symptoms. Stable condition. Continue taking over the counter Prevacid oral capsules, 1 every day.
Patient is instructed to follow up in 3 months. Labs will be obtained prior to visit.
What CPT® code is reported?
A patient presents to the office with dysuria and lower abdominal pain. The physician suspects she has a UTI. A non-automated urinalysis is done in the office and is negative. UTI is ruled out
for the final diagnosis.
What CPT and ICD-10-CM codes are reported?
PDF + Testing Engine

Testing Engine
PDF (Q&A)

